
For a decade, the question was whether to take risk. Now it's whether your measurement infrastructure can keep up.
About 1,300 medical group executives gathered at AMGA in Las Vegas last month. Most have already committed capital to value-based care. The strategic debate is over. A new one is starting.

What most observers are still getting wrong
VBC keeps being discussed as a strategy problem: risk appetite, contract design, care model transformation. That was the problem of the last decade.
The next decade's problem is operational:
For most health systems, the answer is no. The gap is $2-$8 million annually for systems with 200-2,500 physicians. We defend that number below.
What AMGA 2026 made harder to ignore
Stephen Nuckolls, CEO of Coastal Carolina Quality Care, summed it up in the most candid VBC session of the conference: VBC was sold on a clear set of promises. For many organizations, the operational reality has consistently fallen short. (Creyos coverage)
He didn't argue VBC was wrong. He argued execution is hard in a specific, regulatory complexity way. Three shifts make it concrete:
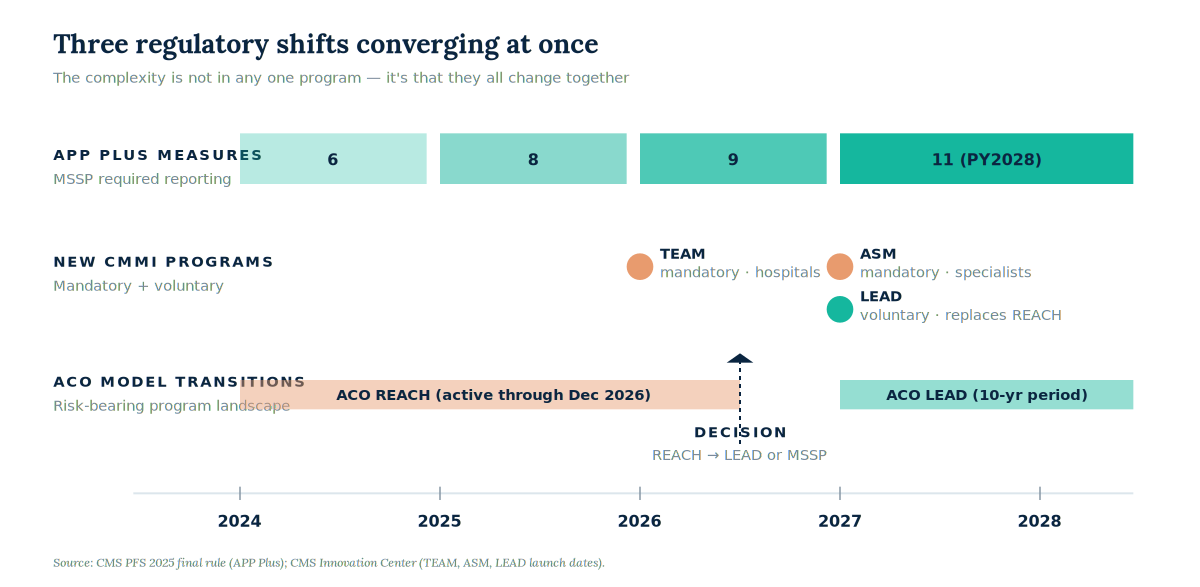
- APP Plus is expanding fast. Six measures in PY2025, 11 by PY2028. The CMS Web Interface is gone. eCQMs or Medicare CQMs are required across the ACO's full attributed population, including non Medicare patients. (CMS PFS 2025)
- The program landscape multiplied. REACH winds down at the end of 2026. LEAD launches in 2027 (10-year period). TEAM became mandatory in January 2026. ASM launches in January 2027. These are parallel systems, not additions to MSSP.
- The destination keeps moving. ACPT is producing systematically lower benchmarks. LEAD's risk adjustment specs are unpublished. Systems are making 10-year commitments against rules that may change inside the agreement period.
The pattern: more measures, more models, and more moving parts than legacy reporting teams were built to handle.
Why this matters more than the AI conversation
At AMGA this year, AI was no longer being argued against. The questions were about implementation.
But almost all the deployed AI discussed (ambient scribes, clinical decision support, diagnostic imaging) lives in the clinical and documentation layers. That's useful, but not where VBC performance is won or lost.
The AI that will move VBC performance lives in a layer the conversation is barely touching: measure trajectory, variance detection, episode cost analytics, and predictive identification of measures about to miss benchmark. Different buyers (CFOs and CMOs, not CMIOs). Harder data. ROI in shared savings, not clinician time saved. We expect this to take most of the field by surprise.
Where Healthmonix sits
We've been building toward this for 3 years. PrismIQ is purpose built for the measurement infrastructure problem we're describing: APP Plus, TEAM, ASM, and MA performance, reconciled to CMS rules, surfaced in time to act.
The first questions our customers ask are almost always the same:
- "Can we see, in 1 view, where we're off trajectory across MIPS, MSSP, and MA?"
- "Can we tell, with enough lead time, which providers will pull our composite score below threshold?"
PrismIQ answers these at the level of individual providers, measures, and episodes — not just year end.
Two case studies. Same pattern.
Esse Health (St. Louis)
Independent primary care. Integrated PCPs with hospital medicine, redesigned compensation. Result: $100+ PMPM pilot savings.
Possible only because they could see outcomes degrading early enough to justify the redesign. That's measurement infrastructure.
Lexington Clinic + CommonSpirit (Kentucky)
"People+ Model" across 7 EDs. Result: 80% reduction in LWBS, 55% reduction in door to provider time.
Possible only because they could measure the right things on a cadence that allowed intervention before problems hardened.
The $2-$8 million, decomposed

- 1MIPS bonus capture: $1M-$3M. Without integrated cross payer analytics, organizations capture 20-25% of available bonus. With it, they capture 70-80%. A 1,500 physician group gains roughly $1-$3 million annual differential.
- 2ACO shared savings: $0.5M-$3M. Variance and trajectory analytics drive higher shared savings per beneficiary than retrospective composite reporting. This is supported by CMS PY2023 data and NAACOS analyses.
- 3Episode cost exposure: $0.5M-$2M. TEAM, ASM, and MIPS episode-based cost measures introduce growing exposure for organizations that can't model episode level variance.
Note: This is our estimate, not a published benchmark. Methodology paper coming Q3 2026.
Three predictions for AMGA 2027
- 1The infrastructure conversation reorganizes. By the end of 2027, "what care model should we build" gives way to "what measurement infrastructure should we have." Most population health platforms competing on care management features reposition or get acquired.
- 2Measurement AI starts moving shared savings. Fewer than 50 health systems will have production AI affecting actual VBC outcomes by mid-2027. Our forecast: those early adopters outperform peers by 1-2 percentage points on MSSP gross savings, visible in PY2027 results.
- 3The Nuckolls framing ages well. "Operational reality has fallen short" will look, in retrospect, like the moment the field stopped arguing about whether VBC was right and started arguing about whether their infrastructure could keep up. That moment is now.
Wondering whether your measurement infrastructure can keep up?
If you left Las Vegas with that question, you're not alone. It's the conversation we're having with health systems right now. Schedule a call.
Sources
AMGA Annual Conference 2026, April 15-18, Mandalay Bay. amga.org
CMS PFS 2025 Final Rule (APP Plus, ACO quality reporting). CMS
CMS Innovation Center (TEAM, ASM, LEAD). cms.gov/priorities/innovation
Smith, E. Creyos Blog, May 5, 2026. creyos.com/blog/amga-2026
Milliman, "Predictability vs. accuracy in MSSP benchmarks," Feb 2025. milliman.com
MIPS capture and ACO shared savings ranges: Healthmonix client engagement data. Detailed methodology Q3 2026.